
Quiet muscles for quiet teeth!
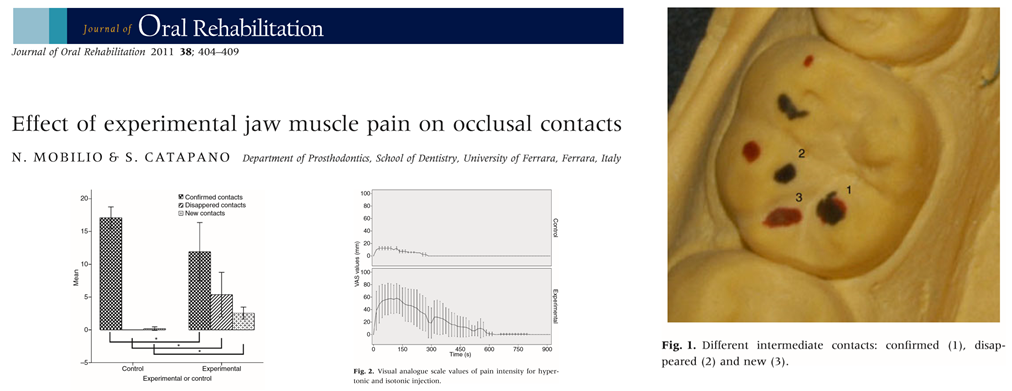
The stomatognathic system abilities to adapt to the morphological changes are individual and variable. Clinical widespread opinion is that some patients “accept” morphological and functional changes related to dental work more easily than others. Most patients easily accept changes in shape, size and dental position; others are able to precisely detect changes, even limited to the tooth surface characteristics, less tolerating prosthesis not perfectly integrated in their oral biology. The adaptation ability is difficult to quantify, since there are no standardized and shared measurement parameters. Regardless of the patient we are treating, it seems still reasonable to limit as much as possible the required changes to its biology. Although it is a scientifically difficult demonstrable concept, we can suppose that an intervention which not affect muscle coordination is an intervention that probably will cause fewer technical complications. Indeed even the tooth not directly affected by rehabilitation procedures will benefit of bridges, crowns and implants that do not alter the chewing patterns; they will suffer the same initial stresses! Applying this concept in a prosthetic projection, we can mention the complication “fracture / chipping of an old reconstruction” immediately following the installation of a bridge, maybe the opposite side of the arch. Another clinical complication provides the appearance of pain in a tooth, following a occlusal change on the contralateral side of the mouth. In both cases, we could hypothesize that the intervention has caused a change in the oral proprioception, triggering a modification in muscles recruitment (then occlusal stress dissipation) that is the cause of the complication which occurred just a few hours away. Concept not widely recognized is that the dental occlusion is not a mechanical situation stable and constant. There are several demonstrations of how the “mechanical” relationship between the dental arches is susceptible to various conditions. For example, the study reported shows that the pain of the masticatory muscles can significantly alter the habitual occlusion (Effect of experimental jaw muscle pain on occlusal contacts. Mobilio N, Catapano S. J Oral Rehabil. 2011 Jun;38(6):404-9). In this dynamic view of dental arches relationship, it is more easily to understand the relation between changes in a dental area and any secondary complications in other areas of the mouth. Accounting that considerations, it seems reasonable to reduce unwanted muscular changes caused by dental treatments.